Type I interferons are made by every cell in the body and are vital leaders of the antiviral battle early in infection. They launch an immediate, intense local response when a virus invades a cell, triggering infected cells to produce proteins that attack the virus. They also summon immune cells to the site and alert uninfected neighboring cells to prepare their own defenses.
https://science.sciencemag.org/content/369/6511/1550
Interferon is een molecuul dat gemaakt wordt als reactie op een virus.
Het interferon activeert mechanismen die het virus in de cel kunnen vernietigen en het waarschuwt andere cellen.
Een corona virus komt binnen. De cel heeft een verdediging. Die leidt tot het maken van interferon en dat leidt weer tot de activatie van afweer genen.
MERS, SARS en dus ook SARS-COV-2 (corona) hebben echter enzymen die de stappen die tot interferon leiden, gedeeltelijk kunnen blokkeren.
Research
Uit wetenschappelijk artikelen blijkt dat mensen die TLR 7 missen of waarbij TLR 7 niet goed werkt, ook het interferon niet goed werkt.
Verder blijkt het type interferon van belang bij de reactie op SARS-Cov-2. Verkeerd interferon kan mensen op de intensive care doen belanden volgen onderstaand artikel.
May 15, 2020 (biolegend)
Interferons During SARS-CoV-2 Infection
The interferon (IFN) response is our immune system’s first line of defense against viral infections. As a critical part of innate immunity, IFNs are produced when cells detect the presence of a virus and signal for cells to create an “antiviral state.” This occurs by the activation of interferon-stimulated genes (ISGs), many of which have direct antiviral functions like blocking viral entry or inhibiting viral genome replication. However, coronaviruses are known to subvert the IFN response. This week, we discuss research that uses transcriptome and single-cell analysis to explore the weakened IFN response in COVID-19 patients and the effects of IFN-based treatments.
Impaired IFN Responses to SARS-CoV-2
Evidence is mounting that the IFN response to SARS-CoV-2 infection is impaired. A recent study examined the immune response in the blood of COVID-19 patients at 8-12 days after onset of symptoms [1]. Using RNA sequencing, the researchers found that in patients with severe disease, expression of ISGs was lower in comparison with patients with mild infection. The researchers also found lower levels of blood IFN protein in severe cases than in mild cases, suggesting that a diminished innate antiviral response to SARS-CoV-2 contributes to disease progression. In support of this, they showed that lower IFN levels were associated with higher plasma viral loads and higher concentrations of disease-driving cytokines like IL-6 and TNF-α.
Another study examined the host transcriptional response to SARS-CoV-2 versus influenza virus [2]. Using ferrets as a disease model, the researchers found that SARS-CoV-2 elicited a significantly weaker IFN response than influenza in these animals. To see if their findings in ferrets were relevant to COVID-19 patients, the researchers then measured blood IFN levels in a cohort of hospitalized patients who tested positive for SARS-CoV-2. They found that hospitalized COVID-19 patients had undetectable levels of IFN proteins, while still exhibiting high inflammatory signatures. Taken together, these data suggest that a weakened IFN response to SARS-CoV-2 allows the virus to cause severe disease. But why do our early antiviral defenses fail against this virus?
A Family of Escape Artists
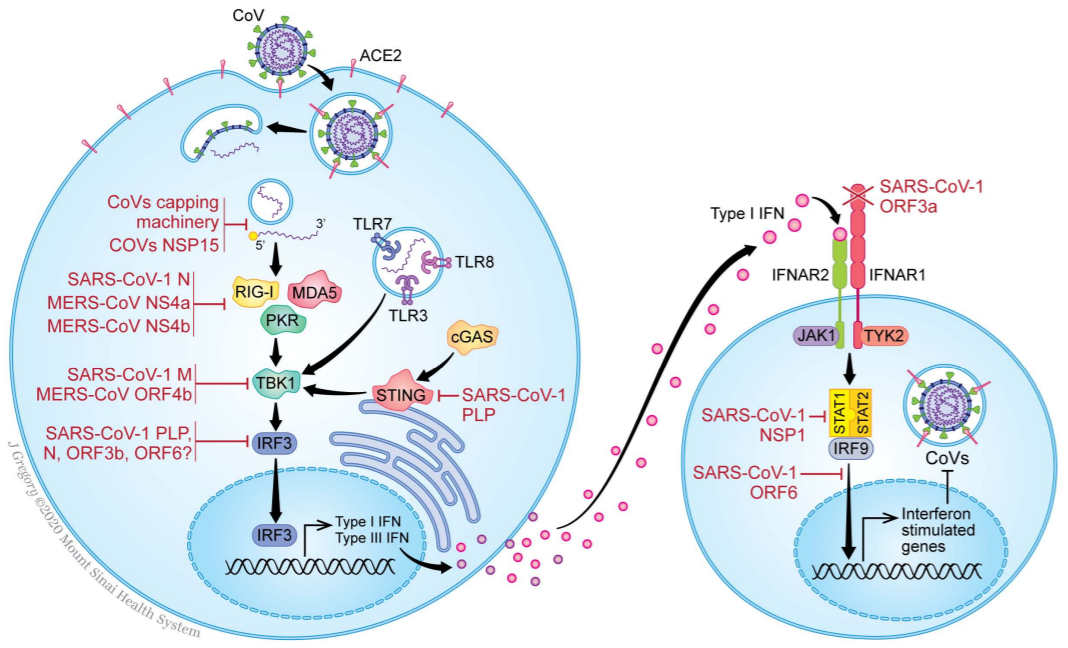
Coronaviruses are known to use a number of strategies to evade the innate antiviral response. The original SARS-CoV is able to avoid detection by pathogen recognition receptors (PRRs) either by shielding its viral RNA or by disrupting PRR activation. Other coronaviruses use their nonstructural proteins to disrupt signaling by interferon regulatory factors (IRFs) – transcriptional regulators of IFN expression. Even after IFNs are produced and start inducing expression of ISGs, coronaviruses have methods to stop these antiviral proteins. One example is the MERS-CoV NS4b protein. This protein is used by the virus to block RNaseL, an IFN-activated nuclease that destroys viral RNA [3].
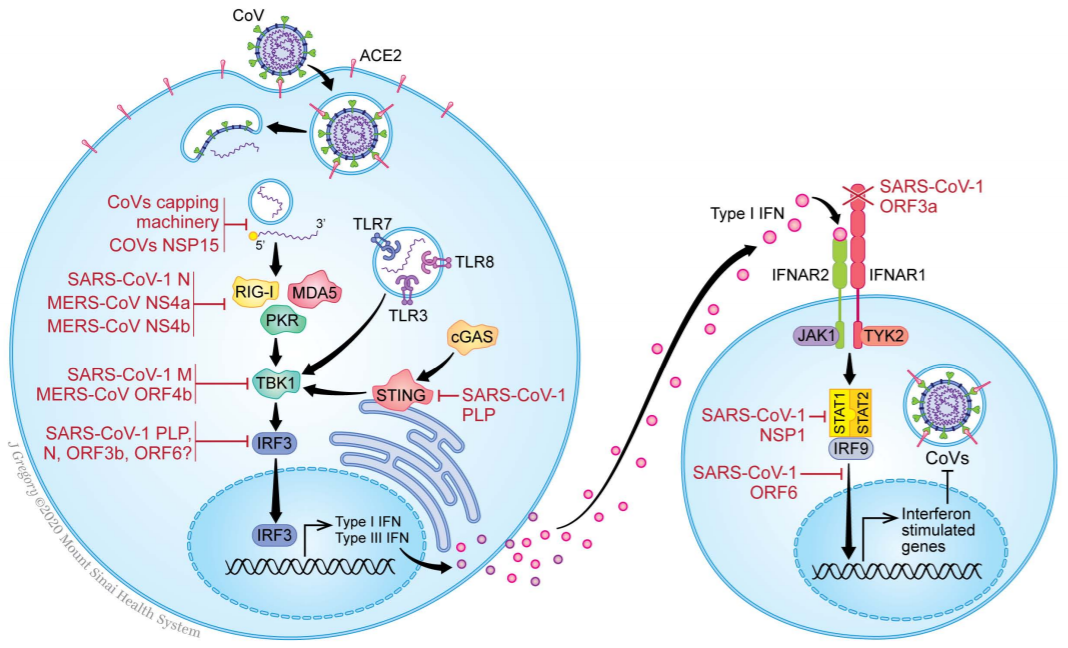 Methods used by coronaviruses to evade the IFN response.
Image source: Vabret N et al. (2020) Immunity, DOI: https://doi.org/10.1016/j.immuni.2020.05.002
Graphic artist: J. Gregory, Mt. Sinai Health System.
Methods used by coronaviruses to evade the IFN response.
Image source: Vabret N et al. (2020) Immunity, DOI: https://doi.org/10.1016/j.immuni.2020.05.002
Graphic artist: J. Gregory, Mt. Sinai Health System.Though the exact anti-IFN mechanisms of SARS-CoV-2 are still unclear, a few studies have revealed protein interactions that indicate how SARS-CoV-2 dampens the innate antiviral response. The SARS-CoV-2 proteins ORF9b and NSP15 have been shown to interact with RIG-I/MAVS and IRF3 signaling, respectively [4]. RIG-I/MAVS and IRF3 are important for triggering the IFN response, so ORF9b and NSP15 likely exert their anti-IFN effects by shutting off these pathways. Thus, SARS-CoV-2 should be no exception in the coronavirus family, a group of viruses that have evolved to be highly adept at escaping innate immunity. These evasion tactics may at least partially explain why some COVID-19 patients develop weak IFN responses to infection.
IFN: A Double-Edged Sword
If the IFN response to SARS-CoV-2 is too weak, the therapeutic answer to this seems straightforward: give patients more IFN. New research cautions that this strategy may not be so simple. A recent study on ACE2, the receptor SARS-CoV-2 uses to gain entry into cells, suggests IFN intervention could actually help the virus replicate. Using single-cell RNA sequencing data, Ziegler et al. characterized human and animal cells expressing ACE2 and found that ACE2 mRNA was often co-expressed with ISGs in the same cell types [5]. This led the researchers to hypothesize that ACE2 expression was also controlled by IFN signaling. Indeed, treatment of human airway epithelial cell cultures resulted in ACE2 mRNA and protein upregulation, indicating that ACE2 itself is an ISG. This means that treating COVID-19 patients with IFNs has the potential to increase infection by stimulating higher expression of the virus’ receptor.
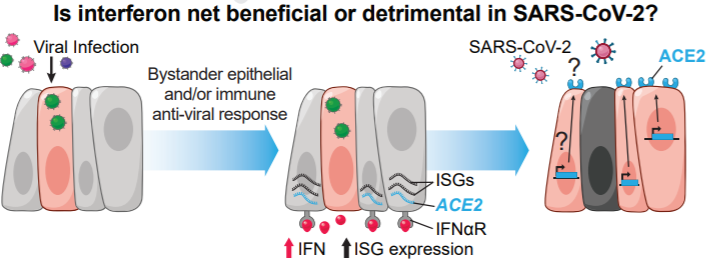 IFN stimulation may upregulate ACE2 expression and increase SARS-CoV-2 infection.
Image source: Ziegler et al 2020 Cell, DOI: https://doi.org/10.1016/j.cell.2020.04.035
IFN stimulation may upregulate ACE2 expression and increase SARS-CoV-2 infection.
Image source: Ziegler et al 2020 Cell, DOI: https://doi.org/10.1016/j.cell.2020.04.035IFN-based treatments may therefore be a double-edged sword. Though anecdotal evidence suggests IFN therapies could worsen SARS disease [6], a more precise application could be effective. Timing of IFN intervention may be a key determinant of its success, since studies in mice have shown that early, but not late, IFN treatment could protect animals from coronaviral disease [7, 8]. Additionally, results from a recent phase II clinical trial demonstrated the effectiveness of IFN, if it was combined with the antiviral drug lopinavir, in shortening recovery time from SARS-CoV-2 infection [9]. Perhaps the added benefit of lopinavir’s direct viral inhibition is enough to overcome IFN’s off-target effects.
As the number of potential COVID-19 therapies under investigation continues to grow, learning more about the virus and its disease will help scientists refine our approaches to treatment. Understanding why therapies work – or situations in which they may fail – starts with knowing the basic science.
If you’re studying innate and adaptive immunity against SARS-CoV-2, learn more about the TotalSeq™ workflow and how multimodal techniques for cellular phenotyping can help you characterize immune responses to viral infections.
References
- Hadjadj J et al. Impaired type I interferon activity and exacerbated inflammatory responses in severe Covid-19 patients. bioRxiv (2020). DOI: 10.1101/2020.04.19.20068015
- Blanco-Melo D et al. Imbalanced host response to SARS-CoV-2 drives development of COVID-19. Cell (2020). DOI: 10.1016/j.cell.2020.04.026
- Vabret N et al. Immunology of COVID-19: current state of the science. Immunity (2020). DOI: 10.1016/j.immuni.2020.05.002
- Gordon DE et al. A SARS-CoV-2 protein interaction map reveals targets for drug prepurposing. Nature (2020). DOI: 10.1038/s41586-020-2286-9
- Ziegler C et al. SARS-CoV-2 receptor ACE2 is an interferon-stimulated gene in human airway epithelial cells and is detected in specific cell subsets across tissues. Cell (2020). DOI: 10.1016/j.cell.2020.04.035
- Lei J et al. CT Imaging of the 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology (2020). DOI: 10.1148/radiol.2020200236
- Kindler E et al. SARS-CoV and IFN: Too Little, Too Late. Cell Host and Microbe (2016). DOI: 10.1016%2Fj.chom.2016.01.012
- Channappanavar R et al. Dysregulated Type I Interferon and Inflammatory Monocyte-Macrophage Responses Cause Lethal Pneumonia in SARS-CoV-Infected Mice. Cell Host and Microbe (2020). DOI: 10.1016%2Fj.chom.2016.01.007
- Hung I et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, phase 2 trial. The Lancet (2020). DOI: 10.1016/S0140-6736(20)31042-4